Antegrade Colonic Enema (ACE) stoma is an opening in the abdomen which, via a surgically constructed channel, opens directly into the caecum. The Antegrade Continence Enema or ACE is a way of managing bowel emptying at a convenient time each day, and should reduce both constipation and soiling. It can be used for patients with the following conditions:
What is an ACE?
The ACE procedure allows washouts to be given directly into the first part of the large bowel to empty it of faeces (antegrade colonic enemas), and as a result promotes continence and or relieves constipation. Complete faecal continence cannot be guaranteed, but if the procedure has been recommended by your Consultant it should improve the present situation.
The stoma does not need an appliance (bag). The stoma is later catheterised intermittently to allow the administration of washout fluid/enema.
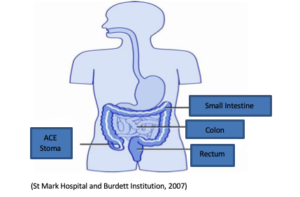
(St Mark Hospital and Burdett Institution, 2007)
What happens before the operation?
Before your child comes in for the operation, you may want to come to the hospital for a pre-admission clinic. More details about this are in your admission letter. You will already have received information about how to prepare your child for the operation. Your Consultant and Anaesthetic will visit you to explain the operation in detail, discuss any worries and explain options for pain relief after the operation. If your child has any medical problems, particularly allergies and constipation, please tell the doctors about these. Please also bring in any medicines your child is currently taking.
Your child may need to have his or her bowel prepared for surgery. This means it will need to be empty of poo. Your child may need to take some medicine (or have an enema if he/ she has an existing bowel problem) before the operation. During this bowel emptying process, your child will not be able to eat any solid food and only drink clear fluids.
What does the operation involve?
The Surgical procedure involves using the appendix as a catherterisable, non-refluxing tunnel from the caecum to the abdominal wall, resulting in a stoma which does not discharge faecal fluid or wind.
If your child has a suitable appendix the surgeon will use this, but if the appendix is absent or unsuitable the channel will be created using intestine. This will be discussed.
Immediate post – operative period
The majority of children undergoing this procedure will return from theatre with an intravenous infusion (drip). There will be a tube in the stoma which will remain for 4-6 weeks.
Your length of stay in hospital will vary depending on the surgery required and your child’s underlying problem. You and your child will be taught how to perform the washouts before you are discharged home, which are normally started 3-4 days following surgery.
A further hospital visit will occur at 4-6 weeks, when you are taught how to insert a catheter into your ACE.
Washout and Enema Regime
There are a number of different medications that can be used for washouts. These are usually diluted with saline (salt water) followed by a salt water ‘flush’. Some children just use saline without any medications at all.
The medications help your bowel contract and push the stool along the intestines and out of the rectum. The saline flush helps to push the medicine and the stool along more quickly. If problems occur between washouts then you will need to change to a different medication.
The amount of washout and saline flush will depend on your child’s age, weight and how effective they are. The total volume of solution used is 10mls-50mls/kg of body weight. We usually start with a volume of 20mls/kg and seldom need to increase this beyond 30mls/kg
Initially the washouts should be done on alternate days – however this may be increased or decreased on the individual’s needs.
Each washout should take approximately 20-45 minutes from start to finish. It is very useful to keep a diary including the washout solution used, length of time the procedure takes, result, record of any accidents/soiling episodes and when the occurred in relation to the washout.
Performing a washout
Everybody’s bowels are different, and there is no way of predicting what will work best. Most people find it convenient to irrigate the ACE in the evening. It does not matter what time of the day the ACE is performed, as long as it is done at approximately the same time each day. Half an hour after a meal is a good time, as the colon often has increased activity after a person has eaten and so maximises the likelihood of good bowel clearance. The bowel has the best chance of establishing a pattern if times are not varied too much.
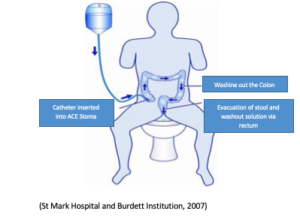
(St Mark Hospital and Burdett Institution, 2007)
Signs of constipation
There are several signs that may indicate that your child is constipated. These include:
It may also be helpful to have some oral medication (Movicol, Senna or lactulose) to help soften the stools. It is also important to ensure that your child is drinking enough water.
Potential problems and solutions
It is not unusual for the stoma to shrink a little following surgery. This can sometimes result in difficulty in passing the catheter. If this does happen insert the smaller catheter you will have been given to stretch the stoma, remove it once it is in and try to pass the regular sized catheter. If this fails continue to use the smaller catheter and contact the Urology CSN Nurse or your Consultant.
It might help to leave a stopper in or a catheter with a stopper in the end of it. Very occasionally the stoma may need to be stretched (dilated) under an anaesthetic. To try to prevent this problem from occurring, you should leave a stopper in the ace or ensure you insert a catheter regularly.
Some children complain of abdominal pain/cramps, dizziness and/or nausea when starting the washouts. This is usually very temporary and resolves as they become familiar with the procedure. It may be related to the strength, volume, temperature and or/speed of the washout solution and you should discuss this with our urology CSN Nurse or your consultant.
This often occurs in the first few weeks while establishing a routine. Never repeat the procedure within 24hrs if no result is obtained. Contact the urology CNS for advice. If the result is delayed or soiling occurs between washouts, contact our urology CNS Nurse for advice about altering the washout regime.
Do not perform the washout contact the hospital for advice before recommencing the washout regime.
Further Support
There are no support groups specifically for children who have an ACE, but the following organisation may be able to offer advice and support.
Association for Spina Bifida and Hydrocephalus (ASBAH)
42 Park Road
Peterborough PE1 2UQ
Tel 01733 555988
Website: www.shinecharity.org.uk
ERIC: The Children’s bowel and bladder charity.
International Children’s continence Society (ICCS)
For further information please contact:
If you have any questions or problems either before or after the surgery, please do not hesitate to contact, Clinical Nurse Specialist, Paediatric Urology, on 020 7580 4400, 10838 (09:00 – 17:00 Monday to Friday) or email at: [email protected]
For Out of hours: Contact our Paediatric Site Practitioner via the switchboard on: 02075804400 ex 10843
